

Colorectal cancer (CRC), also known as bowel cancer, colon cancer, or rectal cancer, is the development of cancer from the colon or rectum (parts of the large intestine).
 1. What is the colon?
1. What is the colon?
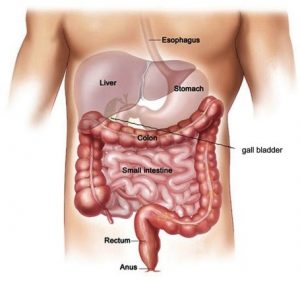
Large Intestine or Colon is the widest part of the intestine which measures about 150cm in length. It starts at the right lower part of the tummy & ends at the anal opening, which is the narrowest part controlled by a muscular ring that acts as a sphincter to hold gas & feces from being escaping without knowledge.
2. What Does The Colon Do?
The food taken is converted to liquid feces of up to 1 liter & colon absorbs water & sodium and forms 150-250ml feces which is expelled. It also produces some good bacteria. When food is taken it may be removed as early as four hours or as slow as four days.
3. What is Colorectal Cancer?
The word cancer is commonly used to describe the dangerously spreading Growth of the inner lining membrane of Colon, Which grows uncontrollably, spreads wherever it likes at the expense of the host. Colorectal cancer is one of the commonest cancer affecting both males and females at varied ages. Though it frequently is seen among the older age group, the younger age group are also can be diagnosed with it. It is a multifactorial disease.
The Importance of Proper Surgery clearing cancer gives excellent results in the prevention of Recurrence & spread.
3.1 Incidence:
Colorectal Cancer is the most common cancer in Malaysia. Third most common cancer in Men & Second in Females. It is the fourth leading cancer death in the world.
80% of cancers are seen among individuals aged 50 years old and above. Most incidence occurs among the age group of 60–69 years old. Most Malaysians often come once the cancer is at a later stage. Western guidelines recommended colorectal cancer screening to start at the age of 50 years to detect Cancer at an early stage. In Malaysia, there is no nationwide, population-based screening for colorectal cancer except for symptom-based evaluation.
| Life Time Risk for Chinese Male. | 1.27 |
| Life Time Risk for Chinese Female | 1.33 |
| Chinese | 28,8/100,000 |
| Malays | 11/100,000 |
| Indians | 14/100,000 |
| Males | 24.16 |
| Females | 18.14 |
3.2 Who gets it?
Both men & women are nearly equally affected, after 50 years old. The average age of diagnosis is 68 years old. Unfortunately, right-sided colon cancer is frequently seen in the younger age group of 20-39 years old.
3.3 What Causes Colorectal Cancer?
Multiple reasons:
a) Can Be hereditary-Genetic. ”Adenoma-Carcinoma” sequences. Most cancer starts as adenomas & most of them are seen on the left side. Hence DETECTION OF ADENOMA IS THE MAIN CRITERIA OF ENDOSCOPY.pts diagnosed as Familial Adenomatosis Polyposis (FAP) are at 100% risk at the age of 40years, though its incidence is around1%
b) Hereditary Non-Polyposis Colon Cancer Syndrome (HNPCC, Lynch syndrome) has 80% lifetime risk and the age of diagnosis is 45yrs. Patients who had Renal/Bladder & Uterine cancer also at risk of developing Colon cancer. Adenoma of more than 1 cm has a risk of 10%, 2-3Cm; 10-15% of developing cancer & More than 3cm has a risk of local spread.
c) Inflammatory Bowel Disease such as Crohn’s Disease & Ulcerative colitis which presents as loose stools to bloody Diarrhea, Those aged 20 years old has a risk of 15-20% and those at 30 years old are at of developing cancer.
d) Others
OBESITY- doubles the risk & will present late stages & poor results. SEDENTARY LIFE /Smoking/Alcohol of even 30G increases the risk.
e) Diet high in Red Meat ( Haem & Nitrosoamine Compunda) & Animal fat is proven risky.
Diet rich in whole grains, Yoghurt, Vegetables, Cereal fibers, fresh fruits, Folic acid & calcium intake reduces the risk.
Drinking High Fructose Corn Syrup (HFSC) has increased risk. (An experimental study shows daily intake of 20 G of HFSC =1 soda increases the development of Polyposis & dysplasia in Mice.) The fructose is converted to Fructose 1 phosphate which activates Glycolysis & increased synthesis of fatty acids which supports the growth of tumors.
 4. What are the earliest symptoms?
4. What are the earliest symptoms?
The symptoms of cancer depend on the part where it starts.
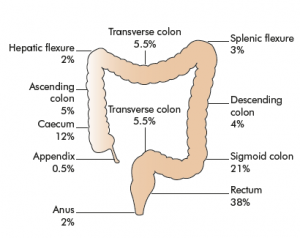
Colon has a variable width, largest in the right side, and rectum then narrower in the anus.
The symptoms depend on the luminal size. If the tumor is near the narrow tube person will have early symptoms due to early blockage. Also what type of tumor, soft fleshy tumor bleeds early which is painless if small quantity presents as chronic Anemia. Hence monitoring Hemoglobin level regularly and if it decreases, it should be assessed properly is of utmost importance. Patients may be brought to the hospital because of bleeding which can be painless and heavy. Many come with syncopal attacks with low blood pressure.
Right-sided cancer is difficult to find out as the symptoms are very vague can be present with swelling. Loss of weight/ /General weakness/which may be due to Anaemia caused by long-standing Blood loss from the bleeding tumor which is very minute mostly from right-side colon cancer and also from Transverse –Horizontal part of the colon.
Change of Bowel habits, bloating of tummy, altered bowel habits-is frequent. Loose small quantity watery stools followed by Constipation is common in Left side cancer.
The patient feels incomplete defecation –a feeling that still some feces is retained in the rectum is common in Rectal cancer, Pain,tape-like stools, Bleeding & need to force are the symptoms in cancer of anal canal. Many patients would have experienced any of these symptoms but do not consult as they feel it is of minor significance, but by the time they present the growth would have involved more than half of the circumference, unless Bleeding.
Some patients consider the Bleeding as from PILES & take nonspecific medication. Lack of awareness/overconfidence/non Acceptance leads the growth to grow to a large size or spread away.
The rest of the symptoms are mostly due to the spread of cancer and its complications.
- Some people can feel the swellings in the tummy.
- Sudden Abdominal Squeezing Pain /Bloating/Vomiting in case Intestines are Blocked by the tumor
- Some can come with yellowish Eyes & urine (Jaundice-Spread to Liver) also a late phenomenon.
- Some Tumor may rupture & pose life-threatening complications
- Spread to Urinary Bladder/Uterus & nerves causing Intense pain
Tummy distention may be slow & Progressive indicating fecal/gas/Fluid accumulation all of which are seen in late cases. Simple Nagging cough for months may indicate spread to the lungs also shortness of breath on walking /daily activities indicates accumulation of water in the lungs & spread to lungs. Pain in the back may be from spreading to the bone. Intense headache and vomiting –spread to the brain.
5. What is the best method of finding?
5.1 The gold standard is Complete Colonoscopic with NBI/Advanced Techniques. Finding small adenomas & random Biopsy of the colon can detect early cases.
Proctoscopic Examination of Anus & Lower Rectum by limited Sigmoidscopy in rectal bleeding will help to find nearly 70% of cases of Left colon.
Good Bowel Preparation is mandatory for early detection of Adenomas/Polyps. Patients must understand the importance of clean bowel preparation for Colonoscopy. Two days of low residue diet & taking promptly the bowel preparation medication with a good amount of fluids is of utmost importance to clean the bowel and detect small adenomas. A careful search for the Adenoma under the folds must be done.
5.2 Detecting Microscopic Bleeding In feces indicates Internal Bleed suspicious of Cancer.
5.3 Tumor markers-CEA level is suggestive of cancer.
5.4 Radiological Scan such as USG/CT Scan/MRI/PET Scan is done to study the extent of Disease.
 6. How to treat?
6. How to treat?
SURGERY is the Main Modality of Treatment from Early-stage (1 -3) to late stages.
- May be as minimal as Endoscopic Surgery in very early cases where Endoscopic Excision can be curative Trans Anal Excision; low small rectal tumors can be removed by the anal route.
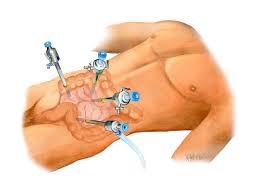
- Laparoscopic surgery offers the best results due to a very good View of Blood vessels /Nerves /Minimal bleeding / minimal Incisions & fast Recovery for Non obstructed cases.
A Good length of Colon removal with all the Lymph nodes removal is mandatory for good results not a small amount of colon.
- If patients come with obstruction, Endoscopic Stenting & release of Obstruction & once the abdominal distension is relieved laparoscopic resection can be offered.
- If the Colon Ruptures causing Fecal Peritonitis or the obstruction cannot be relieved by Stenting or Tumor is bleeding Open Laparotomy & Resection of the tumor with or without Stoma is offered.
- Some patients present isolated liver-lung metastasis, which may require Local Resection of liver & Lung.
- Insertion of Venous Access Port makes it less painful in getting the veins for frequent Blood testing & chemotherapy.
- Total Colectomy with or without Stoma in cases of familial Polyposis is the treatment of choice for prevention.
- Some unfortunate patients where cancer has reached the Anal canal will be benefitted from AP resection (Total Removal Of Colon & Rectum) and permanent stoma.
- The surgical procedure can be combined with Oncological care as Neo Adjuvant/Adjuvant Therapy.
6.2 Stoma:
It is an opening in the tummy wall through which the feces comes out & collected in a bag & Disposed of. Every one considers Stoma as a taboo but it is Life-Saving and many people are living well with the stoma & have become mentors for other new stoma patients.
The stoma is offered only when a good functioning Natural outlet is not possible. It can be temporary or permanent.
Stoma society helps care for new Stoma patients. The Medical Oncology team takes care of Chemotherapy/Targeted Immunotherapy & Radiotherapy.
6.3 Exercise:
Daily exercise boosts one’s immune system & wellbeing.
Family & social support is needed in difficult situations.
7. How long the patient can survive?
The 5-year survival rate for colorectal cancer patients in the United States (all stages included) is 64.4%.
Stage 1- 90%
Stage2- 80%,
Stage3-60%
Stage 4-10%Localized disease: 89.9%
Regional disease: 71.3%
Distant disease: 14.2%
Patients who have undergone Resection of liver deposits also have very favorable survival hence spread to the liver is not an ominous sign.
 Article by:
Article by:
Dr. Anantha Kumar Chinnaswamy
General Surgery, Endo/Laparoscopic Surgery, Certified Medical Impairment Assessor
Sri Kota Specialist Medical Centre